

Varicose veins are dilated and tortuous (repeated twist, bends, and turns) superficial veins. Every vein does not become varicose. On most occasions, the main branches of the saphenous veins are the ones that become varicose.
Main veins in Lower limbs( legs)
- Lower limbs (legs) veins can divide into two systems. They are,
- Superficial venous system
- Deep venous system
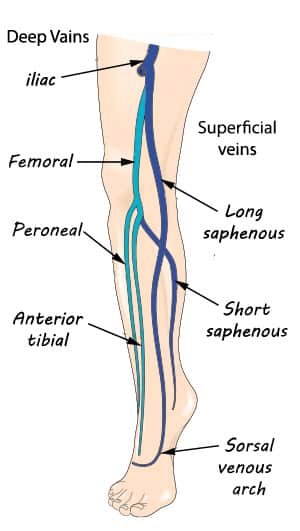
Deep fascia is a thick tissue layer which acts as a base for the superficial fascia. The superficial and deep venous system separates by a deep fascia in the leg.
But at some points, superficial veins pass through the deep fascia and connect to the deep veins. So the two systems connect and communicate.
Usually, the vein which communicates both systems only allows flowing blood from superficial to deep systems. These communicating veins have valves. Those valves prevent blood backflow from deep veins to superficial veins. In deep veins, blood flows upwards from the toe towards the heart. That flow occurs against gravity. Deep veins have many valves that do not let backflow blood due to the force of gravity.
Blood flow mechanism in the veins
In an erect position(standing), venous blood flow occurs from the toes to the heart. This happens due to force, which is produced by a calf muscle pump. That force help to act against gravity. The calf contains soleus muscle. It is a large venous sinusoid (Venous sinusoids is a large capacity of vessels that carries venous blood).
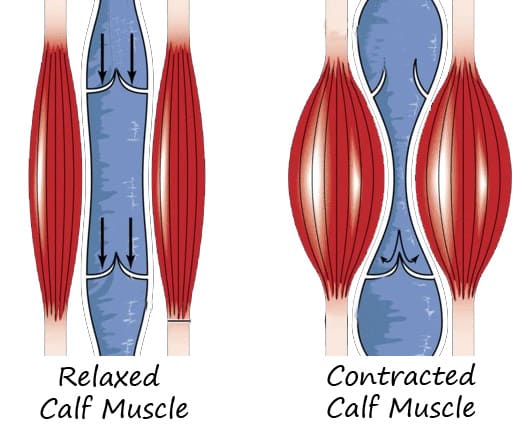
Walking causes calf muscle contraction. Due to this, soleal sinusoids are also compressed. So blood is forced out from the calf veins to popliteal veins and then push towards the heart.
Veins in the calf muscles open in calf muscle relaxation. But blood will not reflux back because veins have valves that prevent blood backflow. After the calf muscle contraction, the deep veins’ negative pressure sucks blood from the superficial veins via the communicating veins. So the pressure in the superficial veins reduces.
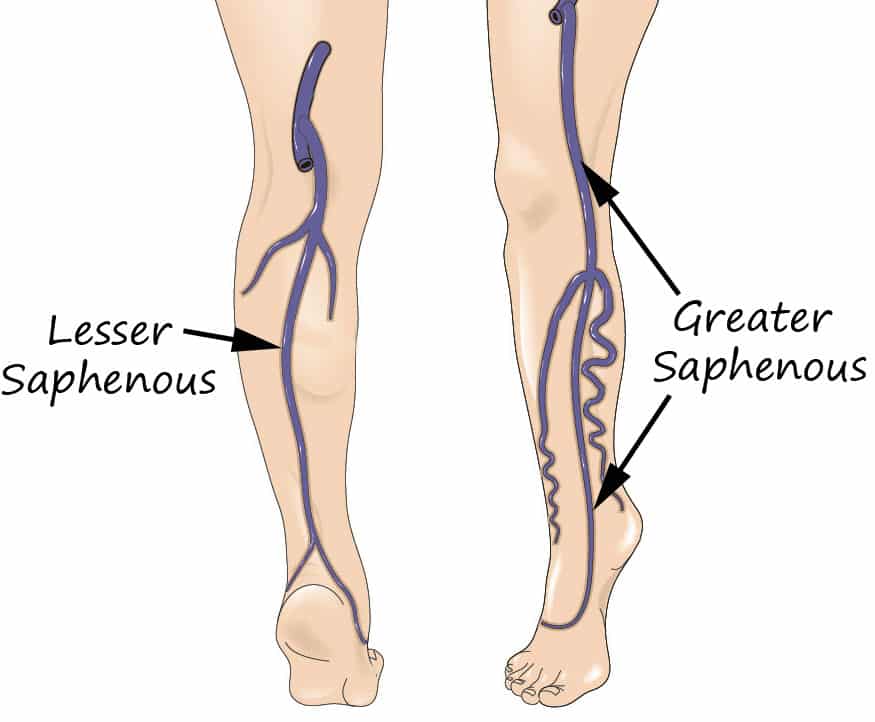
Superficial veins join to the greater saphenous (long saphenous) and lesser saphenous (short saphenous).
Greater saphenous veins end to the femoral vein & Lesser saphenous vein end to the popliteal vein.
Varicose vein
Varicose veins affect all age groups, and most have a clear family history. But it is more common in older people. Also, it is more common in women than in men. In children, it occurs due to congenital vascular abnormality. (abnormality present in the veins since birth)
The varicose vein is common in Europe and North America. But it is less common in Africa and the Far East.
Cause for the varicose veins
The main cause is connective tissue defect and smooth muscle defect in the vein’s wall. (not having a strong coat of smooth muscle in the vein wall)
Predisposing factors for varicose vein
- Age
- Aging increase the incompetency of the valves
- Sex
- Female sex hormones relax the venous wall. Because of that, females are more prone to varicose veins.
- Race
- It is common in Europe and North America
- Weight
- Higher weight adds additional pressure to the veins.
- Height
- Diet
- Side
- (It is common on the left side than the right side)
- Bowel habit
- Occupation
- Heredity
- Clothes
- Prolonged standing
- Venous blood accumulate in the legs and increase pressure in the veins
Types of varicose veins
- There are two types of varicose vein,
- Primary varicose veins
- Secondary varicose veins
Primary varicose veins
The primary varicose vein is the most common type. It is often familial (Relatives might have varicose veins)
Cause for the primary varicose vein is,
- The weakness of the superficial vein wall.
- Especially due to the branches of the saphenous veins does not contain a strong coat of smooth muscle in their wall.
- Lack of a strong wall leads to dilatation of the valve. So valves become incompetent. The backflow of the blood occurs due to valve malfunction.
- Increases in the venous pressure occur due to the backflow of the blood. An increase in the pressure to valves further leads to valves incompetence and condition progress.
Contributory factors for primary varicose veins
- Prolonged standing
- Family history
- The hormonal effect,
- Progesterone in pregnancy has an effect on the veins.
- Aging
Secondary varicose vein
Causes for secondary varicose veins
- Secondary varicose veins happen due to,
- Venous outflow obstruction
- Valve destruction
- Increased blood flow and pressure
- It can see in the arteriovenous fistula. (artery will directly connect with a vein)
- Venous outflow obstruction can see when having
- pregnancy,
- fibroids,
- ovarian cyst,
- enlarged abdominal lymph node,
- pelvic cancer,
- iliac veins thrombosis and,
- retroperitoneal fibrosis.
- The above conditions will cause pressure in the main veins in the abdomen. That pressure compresses the vein. So blood going from legs to heart will obstruct.
- Valve destruction occurs due to the presence of thrombosis (blood clots) in the valves. It can see in deep vein thrombosis.
Symptoms caused by varicose veins
- Disfiguring effect of the veins.
- When the patient is standing for prolonged periods, a dull ache is felt along the veins in the calf muscle and lower leg. The pain will relieve when lying down for 30 minutes and when wearing a compression bandage.
- Night cramps and itching
- Mild swelling of the ankle
- Acute superficial thrombophlebitis. (red, painful, tender lump)
Complications of varicose veins
- Eczema
- Ulceration
- mostly painful wound near the ankle joint
- Lipodermatosclerosis
What are the investigations used to diagnose varicose vein
- Duplex USS
- Standard Doppler Examination
- Venography
- Varicography
Treatment for varicose veins
There are two types of treatment methods used to treat varicose veins. Those are surgical methods and non-surgical methods.
Non-surgical method,
- Apply elastic compression stockings
- Injection sclerotherapy
- Ultrasound-guided foam sclerotherapy.
1. Apply elastic compression stockings
For elastic compression, class one, class two, and class three stockings use.
- Class 1– class one stockings use for simple varicose veins like,
- The feeling of tiredness and heaviness in the legs
- Early venous insufficiency
- Varicose veins in pregnancy
- After sclerosing therapy for the varicose veins
- Mild varicose veins without swelling of the legs.
- Class 2 – class two stockings are used,
- After surgery for varicose veins
- After sclerotherapy for varicose veins
- After deep vein thrombosis
- Marked varicose veins with moderate leg swelling
- When presence healing venous ulcers
In class 2, it applied a range of pressure to the legs. In the ankle, it applies pressure around 30 mmHg, and in the knee, it applies 15 mmHg of pressure.
- Class 3-Class three stockings use for,
- Dermatosclerosis
- Sever venous ulcer
- Swelling of the legs with varicose veins
- Chronic venous insufficiency
In class 3 stockings, around 45 mmHg pressure apply to the ankle of the leg.
2. Injection sclerotherapy
In injection sclerotherapy, directly inject detergent into the superficial veins. Lipid membranes of the veins endothelial cells destroy by this detergent. Initially, veins become shed, and then thrombosis. Then veins become fibrosis and obliteration(sclerosis). The most commonly used sclerosant is sodium tetradecyl sulfate.
After the sclerosing, class one compression stocking use. So it improves sclerosis (adhere veins wall together) of the veins.
- This injecting sclerotherapy method use in,
- minor varicosities and
- recurrence of varicose veins in calf and lower legs.
3. Ultrasound-guided foam sclerotherapy.

For this method, sclerosant converts into foam sclerosants. It is done by mixing air with sclerosant. A three-way tap is used for air mixing.
For foam sclerotherapy, Polidocanol and non recognized detergent are used. Usually, Na tetradecyl sulfate does not use in this method. Under duplex ultrasound scan guidance, a needle is inserted into the vein which needs the treatment. The tops of the saphenous veins are compressed by the ultrasound probe. This helps to prevent the majority of foam from entering the deep veins
- Advantages – both greater and lesser saphenous veins can be obliterated.
- Risk –
- Cutaneous ulceration.
- Deep veins thrombosis
- Escape of the sclerosant into the deep veins cause for it.
- Severe headache after the procedure
- When creating foam sclerosant, the air enters the heart, and the entrance to the brain will cause this.
- Transient blindness
- It will occur due to stroke (poor blood supply to the brain)
Surgical method
- There are three types of surgical method
- Remove the major part of the varicose veins.
- Endovenous laser ablation.
- Radiofrequency ablation.
When a patient has visible varicose veins without having symptoms, usually any intervention is not done. Simple reassurance is enough.
- For the intervention, the patient should have clear indications. Those are,
- the recurrent episode of haemorrhage (bleeding from the varicose sites),
- development of skin changes
- eg: lipodermatosclerosis,
- eg: ulceration
1. Remove major parts of the varicose vein
This method applies to treat when long saphenous and short saphenous veins become incompetent.
- The steps of the surgical procedure are given below.
- As the first step, communicating points of the saphenofemoral and saphenopopliteal junction ligate.
- Then major parts of the incompetent varicose veins trunks are removed. Hence prevent connections with tributaries.
- Then remove tributaries by using a minor cut and teasing those out from under the skin.
- This method can cause damage to the minor nerves.
2. Endovenous laser ablation
- In this procedure, a tube is inserted into the varicose veins by an incision on the skin.
- Then laser therapy is given.
- Due to the laser, heat is produced, and that heat destroys the veins inner layer, and finally, veins wall adhere together. It is a less invasive procedure (it is easier to heal when the cut is small).
- This method is less expensive than Radiofrequency ablation.
3.Radiofrequency ablation
- This method uses radiofrequency waves, and the procedure is similar to endovenous laser ablation.
- It destroys the endothelial lining (inner layer of the veins), and ultimately veins will obliterate.
After above all surgical procedures, it’s a necessity to apply a compression bandage for at least one week to the legs. It improves the outcome and improves venous obliteration (veins adherent).
Pingback: Mucocutaneous Lymph Node Syndrome(Kawasaki Disease) - MedFog