

What is Appendicitis
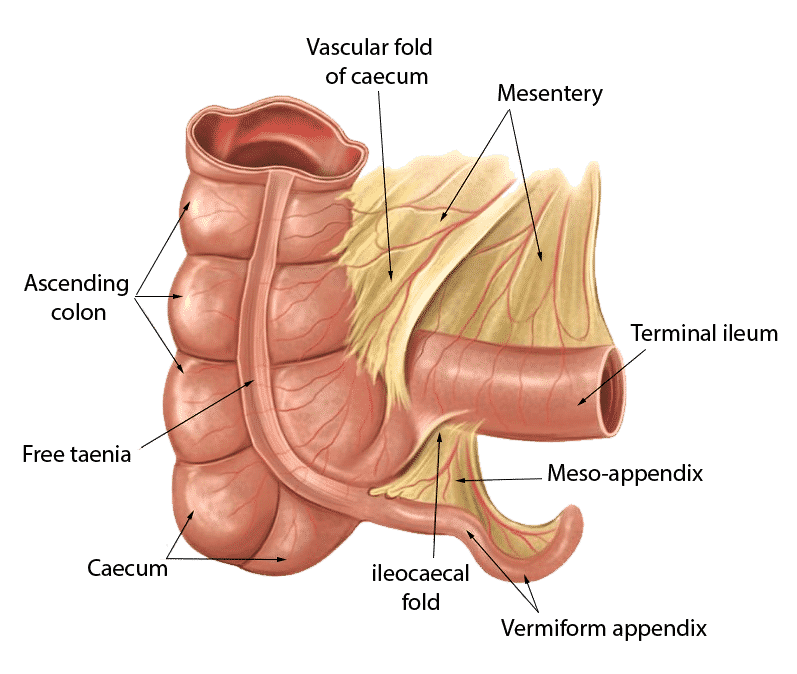
Appendicitis is an inflammation of the appendix. The appendix is a blind muscular tube, which is the undeveloped distal end of the Caecum.
The vermiform appendix is present only in,
- Humans
- Certain anthropic Apes
- Wombat
At birth, the appendix is short and broad at its junction with the Caecum. Around the age of 2 years, it grows to the typical tubular structure.
The appendix varies considerably in length and circumference. The average length is between 7.5 to 10 cm.
The appendix contains numerous aggregated lymphatic follicles. The lymphatic follicles are part of the immune system. But doing an appendicectomy (a surgery to remove the appendix ), there is no discernible change result in the immune function.
Appendicitis can be divided into chronic and acute. But chronic appendicitis is a rare condition. In some cases, chronic appendicitis is not detected until it becomes acute.
- Acute appendicitis is
- Rare in childhood and early adult life
- Peak incidence in the teenage and early 20s
- At the middle age risk of developing appendicitis is quite low.
Before puberty, males and females have the same incidence of appendicitis. But in teenagers and young adults Male to Female ratio for appendicitis is 3:2. After the age of 25, females are more prone to appendicitis.
What Causes Appendicitis?
The appendix is the most frequent site for Carcinoid tumors (Carcinoid cancer). In Carcinoid tumors, occlusion of appendiceal lumen occurs, and it causes appendicitis.
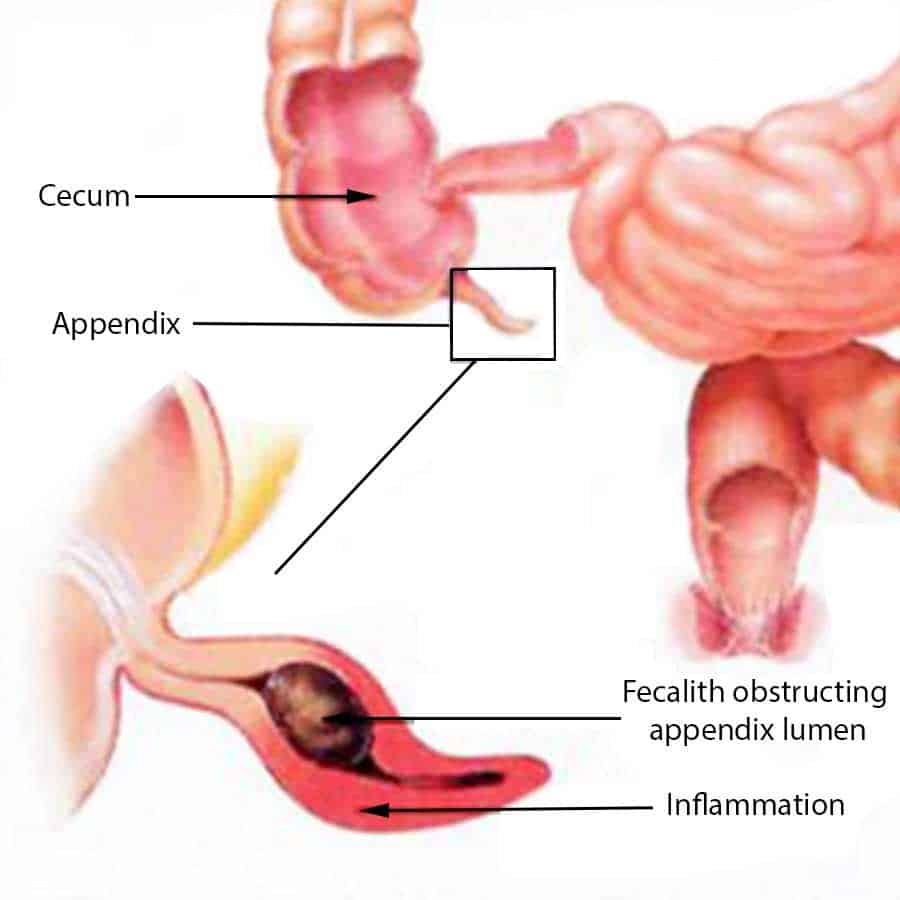
The cause of the appendix is obstruction of its lumen.
- Obstruction of the lumen of the appendix may occur by,
- A stricture or a carcinoid tumor at appendix base
- Threadworm in appendix
- Swollen payers patches
- Fecolith
- Fecoliths are,
- Inspissated fecal materials
- Calcium phosphates
- Bacteria
- Epithelial debris
- Foreign body (mass)
The incidence of appendicitis is the lowest among societies that take a high fiber diet. And it is highest in a refined carbohydrate consumption society.
Stricture of the appendix occurs due to fibrotic band formation after appendicitis that resolved without surgical intervention.
In elderly patients, obstruction of the appendiceal orifice (hall) is caused by a tumor due to carcinoma(cancer) of the Caecum. So it is the cause of appendicitis for most of the middle age and elderly patients.
Also, intestinal parasites (pinworm) can reproduce in the appendix and occlude the lumen.
How Appendicitis Develop
When the obstruction of the luminal orifice of the appendix occurs, continuous mucus secretion and inflammatory exudation occur. It causes intraluminal pressures to increase and obstruct lymphatic drainage. This leads to edema (swelling) and mucosal ulceration development. Then the bacterial translocation and proliferation occur. Aerobic and anaerobic organisms are proliferation in it. In this stage, resolution can occur from antibiotics therapy. But the further progression of the condition causes venous obstruction and ischemia (lack of oxygen) of the appendix wall.
With ischemia bacterial invasion occurs to the appendix, appendix necrosis (cell death ) occur. After necrosed, the appendix may rupture due to bacterial growth. This causes contamination of the interior abdomen from bacteria throughout.
Risk factors for perforation of the inflamed appendix
- There are several risk factors for the inflamed appendix. They are,
- Old age
- Immunosuppression in the patient
- Diabetes mellitus
- Faecolith obstruction of the appendix lumen
- Previous abdominal surgery.
Usually, in appendicitis, intra-abdominal fat will adhere to the inflamed appendix. If previous abdominal surgery was done, that cause to limits the ability of peritoneal fat (intraabdominal fat) to moves around the inflamed appendix wall.
Symptoms of Appendicitis
Initially, vague pain begins in the center of the abdomen. Usually, at first, this may be thought to be due to indigestion and ignored. But after some period (Usually a few hours. But in some times 2 to 3 days) pain shifts to right Iliac fossa (right lower quadrant of the abdomen) and become more severe. This is the typical history of diagnosing appendicitis.
Central abdominal pain due to appendicitis is known as referred pain. (Referred pain is the pain felt in a part of the body other than its actual source). Visceral innervation of the appendix comes from the 10th thoracic spinal segment. The 10th thoracic spinal segment corresponds to the somatic dermatome, which is encircled the abdomen at the levels of the navel. This is the reason for the central pain.
But not all patients will not feel these symptoms. Some patients present with a variety of pain patterns.
- Those are,
- begins, and remain in the right Iliad fossa
- pain is only in the center of the abdomen
- pain on both sides of the abdomen simultaneously
- some patients may not have pain
- Inflammed appendix most commonly lies,
- behind the Caecum (retro caecal appendix). So the pain causes in the left side of the right lower quadrant of the abdomen, and the flank
- hang down into the pelvis and live against the bladder
- hang down into the pelvis and lies against loops of the large bowel. So the patient may mislead with bladder or large bowel symptoms
Before the pain started, some patients may experience constipation for a few days.
- After the onset of pain for a few hours,
- loss of appetite and nausea (feeling of vomiting) occur. Then vomit once or twice
- some complaints of diarrhea which may be misdiagnosed as acute gastroenteritis, especially in children’s
Some may present with symptoms of generalized abdominal pain, nausea, vomiting, sweating, and sometimes rigors. It also can present with intestinal obstruction. So the colic and abdominal distension can occur.
With progressive inflammation of the appendix, coughing, or sudden movement exacerbates the pain in the right lower abdominal quadrant.
When an inflamed appendix present in the pelvis, the typical right lower quadrant of the abdomen pain does not occur. Instead of that, it presents an atypical presentation. It causes suprapubic discomfort and tenesmus (feeling of need to pass stool but can not pass).
In this situation, tenderness (pain when touching) can only be elicited by rectal examinations (index finger will insert to the patient’s anus). If the patient feels pain, he is positive for pelvic appendicitis (If the patient is healthy, he will not feel the pain).
So to identified pelvic appendicitis, the rectal examination is performed on every patient who presents with acute (sudden onset) lower abdominal pain.
Diagnosis of appendicitis
To diagnose appendicitis, a combination of examination findings, symptoms and Laboratory investigations use simultaneously.
- Cardinal features of appendicitis,
- unwell patient with low-grade pyrexia (fever)
- localized abdominal tenderness (pain when touching)
- muscle guarding in the abdomen. (when touched deeply, the abdomen contract abdominal muscle).
- rebound tenderness
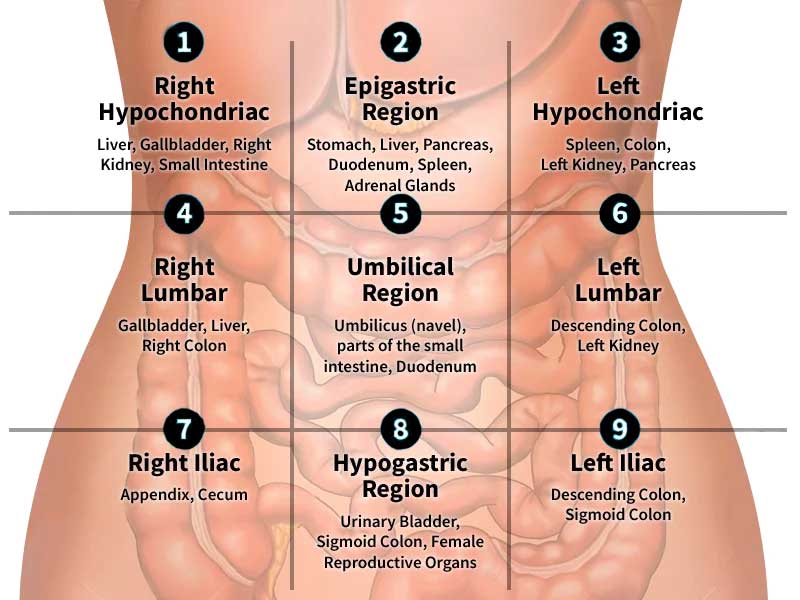
For identifications, purpose the abdomen is divide into nine quadrants.
- In appendicitis, the patient will have
- flushed cheeks,
- low-grade fever,
- elevated pulse rate,
- furring of tongue
- distinctive fetor oris.
- The patient may be kept right hip flexed (bend) when the appendix lies against the Psoas muscle.
- Coughing and sudden movement cause pain if the patient develops peritonitis.
Signs which can elicit in Appendicitis
- Four signs can be elicited in appendicitis. They are,
- pointing signs
- Rovsing’s sign
- Psoas sign
- Obturator sign
But all four signs will not be simultaneously positive in appendicitis.
Pointing signs
- The patient is asked to point to where the pain began and where it moved.
Rovsing’s sign
- Deep touching of the left lower quadrant (left Iliac fossa)of the abdomen may cause pain in the right iliac fossa. (right lower quadrant of the abdomen)
Psoas signs
- The patient will lie with the right hip bend. Because it causes to relief pain if inflamed appendix lies in the Psoas muscle.
Obturator signs
- If an inflamed appendix is in contact with the obturator internus,
- pain can be caused in the hypogastrium area when the hip flexed(bend) and rotated internally.
(Obturator Internus is a name of a hip muscle that originates deep within the pelvis)
How to diagnose Appendicitis
Alvarado Score is use to diagnose appendicitis. It is a combination of symptoms, signs, and laboratory investigations.
- To calculate this score,
- four symptoms,
- two signs, and
- two laboratory tests are used
Positive of more than 6 value out of 10 consider as acute (within a short period of time) appendicitis.
Alvarado Score
- Symptoms
- Nausea( feeling of vomiting) or vomiting-score value 1
- Abdominal pain that migrates to the right iliac fossa-score value
- Anorexia(loss of appetite)-score value 1
- Tenderness ( pain when touching) in the right iliac fossa- score value 2
- Signs
- Rebound tenderness – score value 1
- Fever of 37.3C or more – the score value 1
- Laboratory investigations
- Leukocytosis >10000 – the score value 2
- Neutrophilia>70% – the score value 1
Treatment for Appendicitis
Surgical removal of the appendix is the treatment of appendicitis. Otherwise, the appendix will rupture, and it causes intra-abdominal pus collections. This leads to Sepsis and ultimately to death. So incidental findings of a fecolith in abdominal surgery, appendicectomy will be done before it is inflamed. It is a prophylactic appendicectomy.